
The therapeutic power of the Maggie’s centre: Experience, design and wellbeing – where architecture meets neuroscience
Using Maggie’s as a model, this paper seeks to raise awareness of the constituents of a therapeutic environment, in order to be able to recognise it in any architecture that makes one feel well.
Abstract
In my book, based on my PhD thesis, I investigated the postulate of Maggie's Lead psychologist, Lesley Howells, who maintains that "the synergy between people and place allows psychological flexibility" – that is, a state of mind so flexible in its users that it constitutes a therapeutic environment. In this seemingly calm environment, however, other emotional phenomena that lead people to say, often in tears: "I don't know what this is", "I can't explain it" occur. To find out "what is exactly in a Maggie's Centre that generates a therapeutic power", I decided to explore neuroscience.
By bringing to the reader’s attention people’s behaviours from a biological point of view in response to Maggie’s unconventional architecture, this book explains the ability of the Maggie’s Centre to generate emotional phenomena and, therefore, why we can talk about its therapeutic power. In this, the book critically evaluates Maggie's as a model to be applied to other facilities. The ultimate purpose of the book is to raise awareness in the reader of what a therapeutic environment is, in order to be able to recognise it in any architecture that makes one feel well.
Wanting to deepen my understanding of the impact that the therapeutic environment has on Maggie’s users and how they respond to it biologically, in writing this book I turned to neuroscience primarily for two aspects: that of ‘perception’ (i.e. the experience triggered by movement and in which the brain serves to “predict the future, to anticipate the consequences of action” – scientifically demonstrated by the discovery of mirror neurons) and that of ‘emotions and feelings’ in the experiential process of which, again thanks to movement, the related brain structures are “those necessary for reasoning and to culminate in decision making”.
Although comfort and atmosphere are essential, they are not enough to define Maggie's therapeutic environment. It is only by looking at neuroscience, which can scientifically explain feelings and emotions, and by considering the space neither neutral nor empty, but full of forces that envelop people in an 'embodied experience', that we can understand what generates wellbeing at Maggie's. Aware that I have just begun to delve into neuroscience, in this book I only opened a door to its vast knowledge. However, since other perspectives are needed, this book is an even broader invitation to delve into the subject.
Learning objectives
- Explain how the built environment influences our visual perception and our behaviour
- Facilitate the reader, layperson or not in neuroscience, in understanding the relationship between the two disciplines, highlighting the advantages that this mixture would bring and encouraging greater consideration in future projects
- Understand what the 'embodied experience' is
Introduction
In my book, The Therapeutic Power of the Maggie’s Centre: Experience, Design and Wellbeing – Where Architecture Meets Neuroscience, based on my PhD thesis, I investigated the postulate of Maggie’s psychologist lead, Lesley Howells, who maintains that “the synergy between people and place allows psychological flexibility” – that is, the combination of Maggie’s open and unconventional architecture with the support programme offered by Maggie’s staff generates such a flexible state of mind in its ‘visitors’ (as Maggie’s calls people with cancer, family and friends) that it constitutes a therapeutic environment.1
At the end of my doctoral research, I discovered that the relationship between architecture and psychological flexibility2 of visitors lies in ‘movement’. In a Maggie’s centre, thanks to the openness of the space and the fact that there are no secrets inside the building, people are free to go wherever they want, and therefore they feel active and not passive as when they were in the hospital.
Indeed, during her hospital stay, Maggie Keswick Jencks had experienced first-hand – and understood – that, in hospitals with dark corridors and blinding neon lights, people, sitting tired on plastic chairs, needed a familiar environment, a tailor-made architecture in close contact with nature, able to “empower the patient” through a strategy of “self-help”,3 an active involvement in her own therapy.4 Starting from the belief that “design is a form of care”, Maggie thus gave life to a new concept of healthcare in which architecture plays a fundamental role.
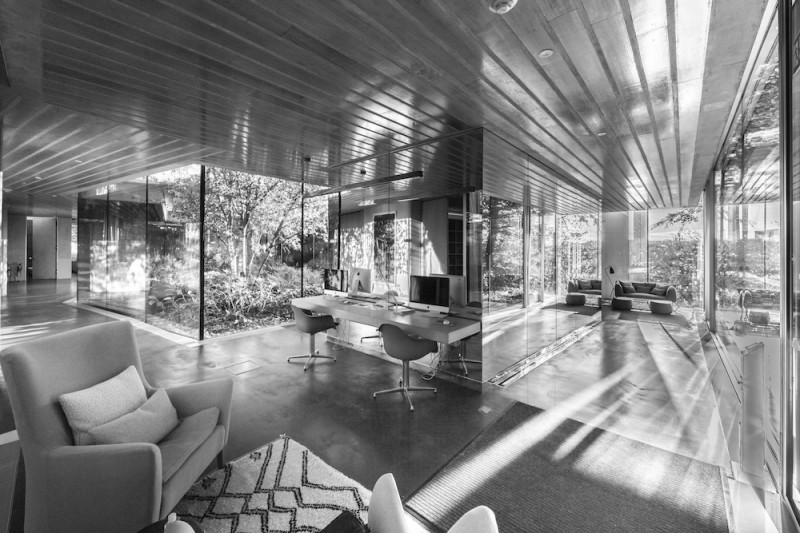 Figure 1: Maggie’s design principle “spatial interaction rather than walls”; Maggie’s Glasgow, 2011. (©Courtesy of Marco Caselli Nirmal)
Figure 1: Maggie’s design principle “spatial interaction rather than walls”; Maggie’s Glasgow, 2011. (©Courtesy of Marco Caselli Nirmal)
Through the design principle of ‘spatial interaction rather than walls’ (see Figure 1), inherent in the architectural brief – the emotional and non-technical programme provided for the commissioned architects – the building accompanies people in the exploration of space; for example, along a curved glass case or a large spiral staircase which, depending on the mood of the day, will orient them towards sociability (kitchen) or privacy (library) (see Figures 2a, 2b, 2c). By moving, feeling connected, even amused by being able to wave from afar, people with cancer feel safe and in control, coming to accept something that was previously unacceptable.

![Figure 2b: Maggie’s ‘movement’ is what connects architecture to psychological flexibility; [Maggie’s Lanarkshire, (2014)]. (©Courtesy of Marco Caselli Nirmal)](https://dev.salus.global/images/uploads/images/_main/2b_copy.jpg)
![Figure 2c: Maggie’s ‘movement’ is what connects architecture to psychological flexibility; [Maggie’s Barts (2017)]. (©Courtesy of Marco Caselli Nirmal)](https://dev.salus.global/images/uploads/images/_main/2c_copy.jpg)
Figures 2a, 2b, 2c: Maggie’s ‘movement’ is what connects architecture to psychological flexibility; [Maggie’s Oldham (2017), Maggie’s Lanarkshire, (2014) and Maggie’s Barts (2017)]; (©Courtesy of Marco Caselli Nirmal)
Similar to Lesley Howells’ analysis, previous studies on the ‘healing architecture’ of the Maggie’s centre had attributed the therapeutic nature of the building to the common action of “generators of architectural atmospheres” – i.e., the combination of materials, light, colour and shape of the buildings5 – together with the good care of the staff. However, no one had gone further in explaining why this interaction was generated, where it came from and, therefore, what was the true source of the therapeutic effects of the Maggie’s centre. In this seemingly calm environment, in fact, other types of emotional phenomena also emerge, which lead people to say, often in tears: “I don’t know what this is,” or “I can’t explain it.”
Wanting to deepen my understanding of the impact that the therapeutic environment has on Maggie’s users and how they respond to it biologically, in writing this book I turned to neuroscience, primarily for two aspects: that of ‘perception’, i.e., the experience triggered by movement and in which the brain serves to “predict the future, to anticipate the consequences of action”6 (scientifically demonstrated by the discovery of mirror neurons); and that of ‘emotions and feelings’ in the experiential process of which, again thanks to movement, the related brain structures are “those necessary for reasoning and to culminate in decision-making”.7
By bringing to the reader’s attention people’s behaviours, from a biological point of view, in response to Maggie’s dynamic space and unconventional architecture, this book aims to explain the ability of the Maggie’s centre to generate emotional phenomena and, therefore, why we can talk about its therapeutic power. In this, the book critically evaluates Maggie’s as a model to be applied to other healthcare facilities. The ultimate purpose of the book is to raise awareness in the reader of what a therapeutic environment is in order to be able to recognise it in any architecture that makes one feel well.
Methods and findings
I sought to investigate the emotional phenomena that occur in a Maggie’s centre and, more generally, to understand how the built environment influences the perception and behaviour of its visitors. Once I had completed visits to 23 centres in Europe and conducted interviews with 12 Maggie’s architects on their interpretation of the architectural brief, which I cross-referenced with Maggie’s co-clients, I immersed myself in three centres (Maggie’s Dundee, Maggie’s Oldham and Maggie’s London Barts) (See Figures 3a, 3b, 3c.), living the life of its visitors for almost four months.



Figures 3a, 3b, 3c: Maggie's Dundee (2003); (©Courtesy of Maggie’s), Maggie’s Oldham (2017) and Maggie’s Barts (2017) (©Courtesy of Marco Caselli Nirmal)
Here, adopting a phenomenological approach – the method for investigating the structure of our lived experience in the world formulated by Edmund Husserl8 – supported by a socio-psychological theoretical background, I undertook my ethnographic work, which consisted of applying four research methods to the field: participation and observation; ‘move-along’; focus groups with visitors; and traditional semi-structured interviews with staff.
With the first method, I observed continuous changes in the spatial arrangement – during the day, Maggie’s staff constantly move the furniture to accommodate the different activities of the support programme – how and where people moved in the building, thus determining the level of ‘therapeuticity’ of the various areas; and how natural light modified the space and influenced people’s perceptions during the day and the seasons.
With the second method, the ‘move-along’ – a sort of ‘architectural tour’ with a photo/diary, i.e., photos downloaded and discussed in a follow-up interview – I was able to see the building through the eyes of the participants, who guided me inside and outside to show me what was most meaningful to them, and as we walked, took photographs in sequence. The aim was to understand how people perceive the building, its ability to generate emotions and feelings in users, and to respond to their expectations by evoking their common impressions. Finally, through the conversations with users (visitors and staff), I learned many personal stories and collected people’s impressions.
Only after leaving the three centres, carefully observing the photographs that corresponded to the emotional responses of my participants, and reflecting on their physical movement during the ‘architectural tour’, was I to understood, as Merleau-Ponty argues, that the space surrounding the body is neither empty nor neutral, but is charged with forces, a dynamic perceptual field, shared by the body and the built environment, where the two merge in an enveloping space “as in a garment”.9 In this immersive space, which Merleau-Ponty calls the “space of experience” or “experiential field”, I was able to identify the hidden structure (see Figures 4a, 4b, 4c) that unconsciously contains people within it, like in a soccer field that, “pervaded by lines of force,” becomes a “structured arena” that guides the player “as if he were not aware of it”.10
Ultimately, as neuroscientist Gepshtein (2020) explains, in the sensory perception of the built environment, dynamics is the decisive factor.11



Figures 4a, 4b, 4c: Maggie’s Dundee (2003), floor plan and section diagrams of the ‘hidden’ structure of the ‘experiential field’ generated by the intricate trussed ceiling, which contains people within imaginary ‘bubbles’ of privacy. (Drawings courtesy of Frank Gehry with diagram by the author); (©Courtesy of Maggie’s)
The commented review of the photos thus showed that the participants’ experience had been ‘embodied’ – that is, they lived a multisensory experience that involves perception beyond the five senses and that makes the moving body become ‘part’ of the space, evident in the continuous change of points of view of the photographs and in photographic details, such as light sources, shadows, reflections and colours. This is where the emotions and feelings experienced by individuals immersed in the dynamic space of the Maggie’s centre originate.12 Indeed, to understand what in a Maggie’s centre activates the ‘movement’ that enables the ‘experiential field’, we must observe the random overlaps produced by “the reflections and accidents of light playing upon a translucent or polished surface”, i.e., the phenomenal transparency. To be sought in those stratifications through which space “becomes constructed, substantial and articulated”13 allowing for an ‘embodied experience’ and facilitating feelings and emotions (“I don't know what this is”, “I can’t explain it”), the phenomenal transparency of the experiential field is the key to understanding the therapeutic power of the Maggie’s centre (see Figure 5).
 Figure 5: In a Maggie’s centre, the random overlaps produced by “the reflections and accidents of light playing upon a translucent or polished surface” (Kepes, 1944),13 i.e., the phenomenal transparency of the ‘experiential field’ is the key to understandi
Figure 5: In a Maggie’s centre, the random overlaps produced by “the reflections and accidents of light playing upon a translucent or polished surface” (Kepes, 1944),13 i.e., the phenomenal transparency of the ‘experiential field’ is the key to understandi
Conclusions
Although architects and neuroscientists still struggle to communicate,14 especially in the healthcare sector, where there is still not enough literature on case studies that correlate the spatial and material characteristics that a healthcare environment must have and the positive effects on users and their immune system,15 with this book on Maggie’s case studies, we can conclude that investigating neuroscience is essential to design an architecture that aims to positively influence the users’ experience.
To this end, in the book, I’ve explored several examples of brain mechanisms – among others, that of ‘mirror neurons’ which, when activated, connect action to perception6 and release empathy that allows Maggie’s visitors, facilitated by the open space, to imitate each other and to transmit wellbeing in an “as if” trigger of Embodied Simulation (ES).16 The “dispositional representations” or recordings of “dormant and implicit” memories which, when they re-emerge, bring to mind not only the painful experience lived at the time of cancer diagnosis but also the emotional reactions of the past.14 The building – a ‘silent carer’ – manages to defeat these by transmitting the message of a ‘safe place’; and, again, ‘wayfinding’ is activated by the “place cells”, located in the hippocampus17 that, together with the “grid cells”, located in the entorhinal cortex,18 form a complete positioning system – a real GPS, which, thanks also to the way the building is designed, allows easy navigation even for newcomers to Maggie’s, highlighting the advantages that the “architecture-neuroscience” binomial would bring, and encouraging architects to consider it in future projects.
Thanks to neuroscience, we also know that the mechanism through which wellbeing arises in people comes from the fusion of ‘mind’ and ‘body’7 and that activating perceptions means generating ‘emotions’ and ‘feelings’, users, too, are encouraged to have a say by judging the built environment based on their emotional response in a ‘new perception of architecture’. While not measurable with certainty, if we increase the level of appreciation and teach users not to take anything for granted, but to be very critical in judging whether a place is ‘good’ or ‘bad’, architects and builders will begin to change the way they design and build, ultimately triggering the process that will improve the built environment.
Although comfort and atmosphere are essential, they’re not enough to define the therapeutic environment of the Maggie’s centre. It’s only by looking at neuroscience, which can scientifically explain feelings and emotions, and by considering the space neither neutral nor empty but full of forces that envelop people in an ‘embodied experience’, that we can explain what generates the therapeutic power of the Maggie’s centre. Despite being acutely aware that I have only just begun to delve into neuroscience, I wanted this book to open a door to the growing knowledge in this field, leaving the reader free to go further in individual research. However, since other perspectives are needed, this book is an invitation to delve further into the subject.
As much as neuroscience is evolving rapidly, there is still much to reveal also about Maggie’s, especially to help other facilities adopt its model, according to Charles Jencks’ will. Given the paradigmatic nature of Maggie’s therapeutic environment, in addition to exploring neuroscience, I strongly encourage architects of future healthcare facilities to adopt this example to make their architecture ‘therapeutic’ and to extend it to other healthcare and non-healthcare facilities, thus contributing to the future ‘construction of health’.
By narrating the therapeutic environment of Maggie’s, seen through the lens of neuroscience, this book takes the discussion to a new level. It’s also helped by the easy accessibility of the building, where visitors can test on themselves the feelings and emotions that Maggie’s visitors experience daily. Understanding first-hand how architecture helps Maggie’s users to cope with illness means understanding the ‘architecture-users-brain’ connection that marks the future of research, theory and practice of design and planning.
Discussion
In recent times, many efforts have been made to improve the quality of healthcare projects, by raising awareness that ‘design matters’ in this sector, too. Despite the improvements made, however, ‘good design’ is still not the message we receive when entering a hospital, which is rather organisational, procedural, institutional and not akin to ‘human care’, which is what characterises Maggie’s. This is because many architects who design hospitals today do not consider the results of scientific studies that demonstrate how the environment affects the emotional state of people, which can be decisive in situations of high stress.19 Indeed, hospital architecture is still considered a field of action for ‘specialists’ who do not like ideas or change.
“They like to do things their own way, without culture or ambition for beauty, but with knowledge that is quickly realised and acquired, and certainly not according to the belief that design is a form of care.”20
This reluctance can only be explained by going back to the origins, namely to their architectural education – fundamental to shape the mindset and ethos of an architect – which, at the time, was certainly not based on studies on the cognitive perception of space or on experiential design. As Sarah Williams Goldhagen argues,21 with very few examples in history (such as the Bauhaus and its descendants), what has always been absent from the design process taught by architecture schools is the experience of the built environment and, what really matters: how people, especially in situations of high stress, react to the built environment, which, as we know, is the goal of neuroscience.
I propose that architecture schools around the world, which already have the responsibility to ensure a better built environment, introduce the subject of the experience of the built environment into their curricula, including courses in biology, cognitive reading of space, and experiential design, which, in the context of healthcare, would help to improve understanding of how psychological wellbeing influences our immune system during illness.15
Engaging students in the difficult topic of health, asking them to design a Maggie’s centre, or providing them with the tools and skills to extend Maggie’s therapeutic qualities to health centres for other pathologies, or to the hospital, so that it’s no longer an organisational, procedural and institutional machine, is certainly a great challenge; however, if we want the architects of tomorrow to be able to design ‘human’ hospitals, the school has a duty to take up this challenge. In this, following the example of similar exercises assigned in the design studios of European architecture schools, the Yale School of Architecture is the last one I know of to have involved students in a pedagogical experience of this type, proposing the Maggie’s model to teach them how to design an architecture that “takes care” and “makes you feel good”, while telling a counter-narrative of the American private healthcare system.
The same challenge is pursued in the hospital sector by the master programme in Architecture and Health at the University Iuav of Venice, which aims to improve the quality of Italian health facilities (hospitals, retirement homes, Alzheimer's centres, etc.), raising students’ awareness of the role of design in healthcare through innovative models (flexible and open layouts), new functional and spatial requirements (silence room, end-of-life communication and organ donation room), and the humanisation of hospital spaces (with art, music, therapeutic gardens) supported by courses in neuropsychology and cognitive neuroscience, biology and botany.
If such efforts were extended to all the architecture schools in the world, I firmly believe that they would automatically be reflected in a better quality of healthcare architecture and in a greater sensitivity of the architects of tomorrow. As per the experience of Maggie Keswick who, by encouraging others, has also helped herself, this will also make us better people.
About the author
Caterina Frisone is scientific director of the Master in Architecture and Health at Università Iuav di Venezia, in Italy.
References
- Howells, L. (2016). Synergy between People and Place, 8 June https://www.youtube.com/watch?...
- Hayes, S. C. (2011). Opening a Door to Psychological Flexibility. ‘Foreword’ in Schoendorff, B., Grand, J. & Bolduc, M-F (eds). La Thérapie d’Acceptation et d’Engagement, Guide Clinique (pp. 11-13) Brussels: de Boeck
- Jencks, C. (2015). The Architecture of Hope: Maggie’s Cancer Caring Centres (2nd ed.). London: Frances Lincoln
- Keswick, M. (1994). A View From The Frontline. Revised and reprinted in 2003 and 2007. https://maggies-staging.s3.ama...
- Martin, D., Nettleton, S. and Buse C. (2019). ‘Affecting Care: Maggie’s Centres and the Orchestration of Architectural Atmospheres’, Social Science & Medicine, 240, pp. 1–8
- Berthoz, A. (2000). The Brain’s Sense of Movement. Boston: Harvard University Press
- Damasio, A. (1994). Descartes’ Error: Emotion, Reason, and the Human Brain. London: Vintage
- Husserl, E. (1982 [1913]). Ideas Pertaining to a Pure Phenomenology and to a Phenomenological Philosophy. First Book: General Introduction to a Pure Phenomenology. Translated by F. Kersten. The Hague: Nijhoff
- Mallgrave, H.F. (2013). Architecture and embodiment. The implications of the new sciences and humanities for design. London and New York: Routledge
- Merleau-Ponty, M. (1963 [1942]). The Structure of Behaviour. Translated by A. L. Fisher. Boston, MA: Beacon
- Gepshtein, S. and Berger, T. (2020). Dynamics of Architectural Experience in the Perceptual Field. 16 January. https://www.youtube.com/watch?v=HI7s8OhZpT4&ab_channel=AMPS
- Frisone, C. (2021). The Role of Architecture in the Therapeutic Environment. The Case of the Maggie’s Cancer Care Centre, Doctoral Thesis, Faculty of Technology, Design and Environment, Oxford Brookes University. https://doi.org/10.24384/0ejy-...
- Rowe, C. and Slutzky, R. (1963 [1956]). ‘Transparency, Literal and Phenomenal’, Perspecta, 8, pp. 45–54
- Eberhard, J. P. (2009). ‘Applying Neuroscience to Architecture’, Neuron, 62(6), pp. 753–756
- Sternberg, E. (2009). Healing Spaces: The Science of Place and Wellbeing. Cambridge, MA: Belknap Press of Harvard University Press
- Gallese, V. (2009). ‘Neuroscienze e fenomenologia’, Treccani Terzo Millennio, Vol. I, pp. 1–32. https://www.treccani.it/enciclopedia/neuroscienze-e-fenomenologia_%28XXI-Secolo%29/
- O’Keefe, J. (1976). ‘Place Units in the Hippocampus of the Freely Moving Rat’, Experimental Neurology, 51(1), 78–109
- Hafting et al. (2005). ‘Microstructure of a Spatial Map in the Entorhinal Cortex’, Nature, 436(7052), pp. 801–806
- Worpole, K. (2009). Modern Hospice Design. London and New York: Routledge
- de Rijke, A. (2018). Interview with Alex de Rijke and Jasmin Sohi, about Maggie's Oldham, dRMM office, London, 2 May 2018
- Williams Goldhagen, S. (2017b). ‘How the Brain Works and What It Means for Architecture’. Interview with Sarah Williams Goldhagen. Interviewed by M. C. Pedersen for Common Edge, 20 July. https://commonedge.org/sarah-w...
Presenters

Event news










Actions to improve urban renewal and health equity
2nd September 2024
A vision for Liverpool: Putting people’s health first
2nd September 2024
Investing in urban renewal and health equity
21st March 2024
Health equity: Marmot Cities
20th March 2024